
Multistage Clinical Trial Phases With Cost Involved New Drug Development Process


Try Before you Buy Download Free Sample Product
 Impress Your
Impress Your Audience
Editable
of Time


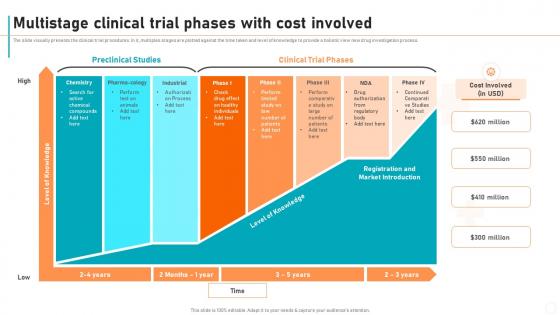
The slide visually presents the clinical trial procedures. In it, multiples stages are plotted against the time taken and level of knowledge to provide a holistic view new drug investigation process.
People who downloaded this PowerPoint presentation also viewed the following :
Multistage Clinical Trial Phases With Cost Involved New Drug Development Process with all 6 slides:
Use our Multistage Clinical Trial Phases With Cost Involved New Drug Development Process to effectively help you save your valuable time. They are readymade to fit into any presentation structure.



FAQs for Multistage Clinical Trial Phases With Cost Involved New
So basically Phase I is just making sure it won't kill you - they test on like 20-100 people to figure out safe doses. Then Phase II bumps up to a few hundred people to see if the thing actually works while watching for side effects. Phase III is the big kahuna with thousands of people where they pit it against whatever treatment already exists. It's kinda like that recipe analogy but honestly, each phase takes forever and costs a fortune. When you're reading about trial results, definitely check what phase they're talking about because Phase I data doesn't mean much compared to Phase III stuff.
The FDA basically runs the show on your trial design - they're setting safety limits, deciding when you can advance phases, picking your endpoints. Each stage needs their thumbs up first. Their feedback will probably flip your protocol upside down, trust me. Patient selection, stats plans, adaptive stuff where you're tweaking mid-trial - they've got opinions on all of it. Here's what I'd do: get those pre-IND meetings scheduled ASAP. Don't make my mistake of finalizing everything then hoping they'll sign off. Start those conversations early and save yourself the headache.
Look, your stats plan is everything in multistage trials - it decides if you stop early, keep going, or pull the plug completely. Set up interim analyses at specific points to check safety and efficacy data. Methods like O'Brien-Fleming help control for multiple testing issues (trust me, you need this). Your biostatistician handles the conditional power calculations at each stage. Oh, and definitely lock down your statistical boundaries upfront - changing them later is a nightmare with regulators. I've seen teams scramble because they didn't plan properly from day one.
So Phase I is all about watching for bad reactions in tiny groups - you're basically figuring out what dose won't kill people. Then Phase II gets messier because now you're tracking both safety AND whether the thing actually works (honestly the worst phase to manage). By Phase III you've got huge patient populations and usually some independent board breathing down your neck, reviewing everything constantly. Oh and regulatory folks can shut you down at any point if things go sideways. Bottom line though - don't even think about recruiting until your safety protocols are bulletproof. I've seen too many trials crash because they rushed that part.
So Phase I is really just about two things - what's the right dose and is it safe enough to keep going? They're hunting for the maximum tolerated dose, which is basically the highest amount people can handle without getting wrecked by side effects. Honestly, at this point it's way more "don't hurt people" than "cure cancer." They'll track the nasty side effects, build out the safety data, and if they're super lucky maybe see some early signs it actually works. The big win? Being able to say "okay, here's our Phase II dose and people can actually handle it" without anyone ending up in the ER.
Dude, it's all about what you're actually trying to figure out. Efficacy testing? Go with response rate or progression-free survival - way faster than waiting around for overall survival data. Dose-finding is different though, you're watching safety plus PK stuff. The mistake everyone makes (me included, honestly) is throwing in like 15 secondary endpoints because they seem interesting. Don't do it. Just muddies everything up. Pick the ones that'll actually tell you if Phase III is worth it. Oh, and double-check your sample size has enough power - sounds obvious but you'd be surprised how often that gets overlooked.
Honestly, the toughest part is juggling participant safety with getting solid data. Your informed consent has to be bulletproof - people need to know the study might shift gears based on what you're seeing. Real-time safety monitoring is where things get stressful because you're constantly deciding whether to keep going or change course. Here's the weird part: maintaining equipoise gets messy when early data hints one treatment's working better. Plus there's this nagging question - if you stop early for good results, are you screwing over future patients who might've benefited from the complete study? Get your safety board's stopping rules locked down first.
So Phase I is pretty straightforward - you only need like 20-100 people, usually through specialist centers or doctor referrals since you're just testing safety. Phase II gets trickier because you're scaling up but still need specific patient types, so the eligibility stuff starts becoming a headache. Then Phase III hits and honestly, it's a whole different beast. You need hundreds or thousands of participants across tons of sites, which means patient registries, social media campaigns, community outreach - the works. The budget and time pressures get intense too. My advice? Start planning your recruitment strategy way earlier than you think you need to.
Honestly? The paperwork will absolutely kill you. Every phase needs mountains of documentation proving you hit your safety targets. FDA wants updated protocols, manufacturing details, all of it - and their review process takes forever while you're bleeding money. Most sponsors don't budget for these delays, which is insane to me. You'll also be tweaking your patient groups constantly based on what phase 1 taught you. Start prepping those transition docs way earlier than feels necessary. And seriously, pad your timeline estimates. The regulatory bottlenecks are brutal but predictable if you plan right.
So basically, adaptive designs let you tweak your trial as it's running based on the data coming in. Pretty genius, honestly. You can bump up sample sizes, ditch treatments that aren't working, or even switch endpoints mid-stream without messing up the science. Think of it as course-correcting instead of flying straight into a data disaster. The real win? You'll stop early if something's clearly not working or if you hit a home run. Plus you can shift resources to whatever's actually showing promise. I'd start by figuring out where interim checkpoints would help most.
Phase IV trials are basically the "real world test" after your drug launches. You get to see how it actually performs when thousands of different patients use it in normal clinical settings - not those super controlled trial environments. Earlier phases miss stuff because of smaller groups and shorter time periods. Phase IV catches rare side effects, weird drug interactions, and long-term effects that didn't show up before. Honestly, it's where you finally see if your treatment holds up. Use this data to update your prescribing info and spot any problems early on.
So basically it comes down to who's writing the checks and calling the shots. Academic researchers run investigator-initiated trials using grant money or whatever their institution can scrape together. Industry trials? That's pharma companies funding and controlling everything. Academic ones usually have tighter budgets and take forever - honestly, dealing with grant cycles is such a pain. But you get more freedom to focus on interesting research questions instead of just hitting regulatory checkpoints. Industry trials move way faster with serious money behind them, though they're laser-focused on getting drugs approved. If you're thinking multistage, figure out your funding strategy early because academic trials often crash and burn when it's time for the next phase.
So basically AI is totally changing clinical trials right now. You've got adaptive designs that can tweak protocols on the fly based on data coming in. Pretty cool stuff. Wearables and phones are tracking patients 24/7 instead of making them schlep to the clinic every few months. Real-world evidence from health records is filling gaps that traditional trials miss. COVID really pushed decentralized trials into the mainstream - honestly they should've been doing this years ago. The biggest advantage? You can spot which treatments actually work way earlier and dump the duds before wasting tons of time and money.
Look, demographics will absolutely mess with your trial if you're not careful. Age matters because older folks process drugs differently. Women get different side effects than men - it's wild how much that varies. Race plays into it too with genetic variants being more common in certain groups. Your recruitment gets biased toward one demographic? Good luck convincing regulators your results apply to everyone else. The FDA's gotten pretty strict about this stuff lately, asking for diversity data upfront. I'd start tracking these factors early and stratify your randomization around them. Trust me, it'll save you so much trouble when they start grilling you about generalizability later.
Honestly, patient registries are game-changers for multistage trials. They help you find eligible participants across phases AND track outcomes way past your endpoints. Find rare disease patients for early phases? Check. Follow those same populations through later stages for real-world data? Double check. The FDA absolutely loves post-market surveillance stuff too. Here's the thing though - don't wait until later to set this up. Get cozy with registry managers during Phase I. Trust me, future you will be grateful when you need that patient data. My colleague learned this the hard way last year.
-
This PowerPoint layout is very helpful from a business point of view, and it's visually stunning too! I'm so happy with this product because it has helped me understand and deliver great presentations.
-
Placing an order on SlideTeam is very simple and convenient, saves you a lot of your time.