


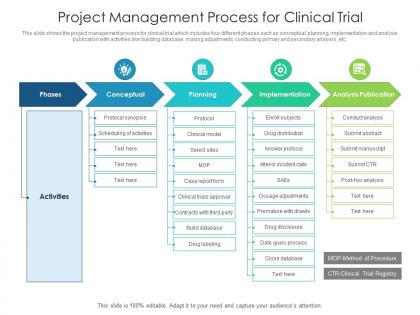
Project management process for clinical trial


Try Before you Buy Download Free Sample Product
 Impress Your
Impress Your Audience
Editable
of Time


This slide shows the project management process for clinical trial which includes four different phases such as conceptual, planning, implementation and analysis publication with activities like building database, making adjustments, conducting primary and secondary analysis, etc.
People who downloaded this PowerPoint presentation also viewed the following :
Project management process for clinical trial with all 2 slides:
Use our Project Management Process For Clinical Trial to effectively help you save your valuable time. They are readymade to fit into any presentation structure.
FAQs for Project management process
So there's five main stages you'll hit: initiation (scope + approvals), planning (protocol and site stuff), execution (recruiting patients through collecting data), monitoring (quality checks), and closeout (analysis/reporting). Planning is honestly make-or-break territory - nail your timeline and risk assessment here or you're screwed later. Each phase has regulatory hoops to jump through, so pad your schedule. Map out your critical path dependencies first. Shows you where things might get messy down the road. Oh, and execution always takes longer than you think it will, just saying.
Start with your endpoint readout date and work backwards - that's your anchor point. Build in buffers for regulatory stuff, patient recruitment, database lock, all that. I always pad things by 20-30% because recruitment is basically guaranteed to be slower than you think. Map out the critical path: site activation, first patient in, data lock, stats analysis. Oh and don't forget seasonal stuff affects enrollment too. Set up quarterly check-ins to pivot if needed rather than crossing your fingers. Keep milestones visible so everyone's on the same page about what's coming next.
Honestly, site coordination is gonna be your biggest nightmare. Every site works differently - some are super organized, others... not so much. Getting them all on the same page feels impossible sometimes. Patient recruitment always takes longer than you think it will. Supply chain stuff gets messy too because you're constantly trying to balance having enough drug without wasting tons of money on overstock. Oh, and data management - sites have different tech setups so that's fun to deal with. Build in extra time for literally everything. I can't stress that enough. Set up your communication rules early or you'll regret it later.
Integrated platforms are a game-changer for trial management - they centralize patient recruitment, data collection, all that stuff. Start with EDC systems for real-time data capture, CTMS for workflow automation, maybe some AI tools for enrollment predictions. Don't try to do everything at once though. Pick your biggest pain point first. Patient scheduling? Regulatory docs? Site communications? Whatever's eating up most of your time. The trick is finding tools that actually integrate instead of creating more headaches. I learned this the hard way - piloted way too many things simultaneously and it was chaos.
Look, risk management is honestly what makes or breaks your trial. Map out everything that could go sideways - recruitment delays, regulatory issues, crappy site performance, data mess-ups. I can't tell you how many trials I've watched crash because teams ignored the obvious risks. During protocol development, start building your risk register. What's the likelihood? How bad would the impact be? Then create backup plans for each phase. Oh, and keep updating that thing as you go - sounds boring but you'll thank yourself later when something inevitably goes wrong.
Documentation systems are your lifeline - set those up first. Automated reminders will save you from missing safety reports and protocol stuff (trust me on this). Train your site staff continuously, not just once at the beginning. Weekly check-ins with CRAs work well, plus monthly updates with the PI. Here's the thing though - everyone tries to catch up on their TMF later and it's a nightmare. Keep it current as you go. Oh, and build compliance into your regular weekly stuff instead of treating it like this separate mountain you'll climb someday. Way less painful that way.
Honestly, you'll want weekly sponsor calls and monthly steering meetings set up from day one - define who does what before things get messy. Quarterly PI meetings too. Dashboards help everyone see enrollment and safety numbers in real-time, which saves you from constant update emails. The relationship stuff matters way more than people think - I've watched trials completely implode when investigators felt ignored during big decisions. Tailor your messages though. What regulators need is totally different from what site coordinators care about. Oh, and figure out your escalation process early so problems don't sit around getting worse.
Okay so budgeting for clinical trials is basically predicting every cost upfront, then watching your spending like a hawk. Site payments, patient recruitment, monitoring visits, lab work, regulatory stuff - the expenses are endless honestly. Always build in 10-15% contingency because trust me, something will go wrong. Most companies have these crazy detailed templates that split costs by phase and site. Finance wants monthly burn rate reports (fun times), so track your actual spending vs what you projected. Oh and start conservative with estimates - asking for more money halfway through is way harder than returning unused funds.
Honestly, you gotta watch enrollment rates and protocol deviations like a hawk. Patient retention is massive too - once people start dropping out, your stats go to hell. Timeline adherence, data quality, safety signals... all that stuff matters. Oh, and query resolution times because those always drag on forever. Site performance is key - look at screening-to-enrollment ratios to see who's actually pulling their weight. Budget variance will make or break you since nobody wants to explain cost overruns. Get your dashboard running early and check it weekly. Trust me, catching problems fast saves your sanity later.
Exit interviews work great, plus regular check-ins during their visits. Anonymous surveys through your trial system too. Honestly, people are way more upfront than you'd expect when you just ask directly - they'll straight up tell you "scheduling was a mess" or "Sarah explained everything perfectly." Document it all in your tracking system and bring up patterns in team meetings. Oh, and actually do something with the feedback when you can. Participants notice when you make changes based on what they said, and it really matters to them.
Honestly, site selection can totally make or break your whole trial. Bad sites = recruitment hell and protocol mess-ups that'll bite you later. I learned this the hard way on a project last year - we picked sites that seemed perfect but couldn't actually deliver patients. Ended up adding like 3 months to timeline. Now I always dig deep into their track record first, especially in your specific therapy area. Yeah, the upfront feasibility work takes forever and feels tedious, but it's so worth it. Trust me, spending that extra time vetting saves you from major headaches down the road.
Honestly, most trial disasters happen because nobody knows who's doing what. Get everyone in a room day one - your stats people, clinicians, data folks, regulatory team. Make them explain their roles and what keeps them up at night. I'm obsessed with RACI matrices for this stuff (sounds boring but trust me). Regular cross-team meetings are clutch so people aren't working in bubbles. The real trick? Create an environment where someone can say "hey, this is fucked" without getting their head bitten off. Psychological safety sounds fluffy but it prevents massive problems later.
Honestly, get your documentation system locked down from day one - don't wing it. Standardized case report forms are a must, and document stuff as it happens, not later when you're scrambling. Version control will save your life with all those protocol changes that always pop up. Real-time audit trails for any edits too. For reporting, stick exactly to what FDA or EMA wants and do regular interim reports. I learned this the hard way - consistency beats everything else. When auditors show up (and they will), you'll be so glad everything's organized and accessible instead of buried in random files somewhere.
First thing - get your reporting system locked down with clear timelines. Twenty-four hours for serious stuff, more time for minor events. Train your site staff hard on this because I've seen studies completely derail when someone doesn't know who to call. Your DSMB meetings need to happen regularly, and document literally everything. Oh, and always overcall causality if you're unsure - better safe than sorry. Set up direct lines between sites and your medical monitor too. You don't want safety issues getting lost in some weekly report that nobody reads until it's too late.
Clinical trial PM is tricky - you'll need specialized stuff like Medidata Rave or Veeva Vault for data management and compliance. The learning curve sucks but pays off. Most teams I know mix those with Monday.com or Smartsheet for timelines, then Slack for day-to-day communication. Oh, and don't forget eTMF systems for document management - regulatory nightmares are real. My advice? Figure out what your team's already using first. Find the biggest headaches and tackle those tools first rather than overhauling everything at once.
-
Excellent template with unique design.