
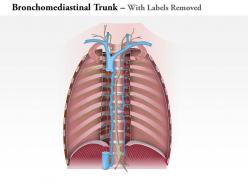
0714 bronchomediastinal trunk medical images for powerpoint


Try Before you Buy Download Free Sample Product
 Impress Your
Impress Your Audience
Editable
of Time


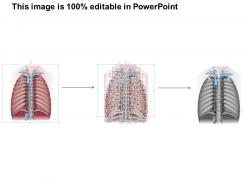
Get above the din with our 0714 Bronchomediastinal Trunk Medical Images For PowerPoint. Your ideas acquire a distinctive character.
People who downloaded this PowerPoint presentation also viewed the following :
0714 bronchomediastinal trunk medical images for powerpoint with all 9 slides:
Our 0714 Bronchomediastinal Trunk Medical Images For PowerPoint get you to grow in confidence. They give you cause to feel good.
FAQs for 0714 bronchomediastinal trunk medical
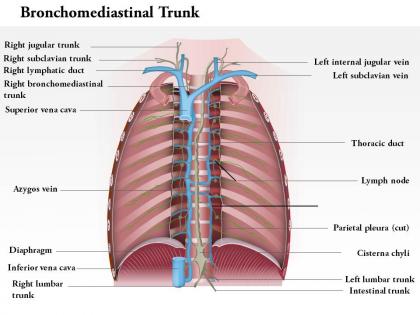
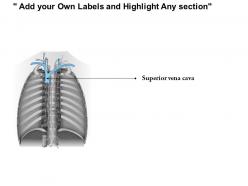
So the bronchomediastinal trunk runs through your superior mediastinum, right along the medial edge of the anterior scalene muscle. It drains into the venous angle where your internal jugular and subclavian veins connect. Right side's pretty straightforward - dumps directly into that junction. Left side? Way more variable honestly, usually connects to the thoracic duct first but anatomy gets weird there between people. It sits behind your clavicle, in front of the lung apex. Oh and it collects lymph from lungs, heart, all that mediastinal stuff - so if you mess it up during procedures, you're looking at some nasty lymphatic issues.
So the bronchomediastinal trunk is basically your lung's lymph highway - it grabs lymph from your lungs, bronchi, and all that mediastinal stuff. Each side works differently though. Right side usually dumps into the right lymphatic duct or straight into the venous angle, left side goes to thoracic duct. Honestly, I always mix up which goes where until I draw it out again lol. It handles all the hilar nodes, paratracheal ones, some anterior mediastinal nodes too. Super relevant when you're trying to figure out how chest infections or cancer spread around.
Okay so the bronchomediastinal trunk basically collects from paratracheal, tracheobronchial, and pulmonary lymphatic vessels - all the big ones draining your lungs and mediastinum. Some upper intercostal vessels dump in there too, plus thymus sometimes. Honestly sounds way scarier than it is - just think of it grabbing everything from that central chest area. Oh and left side drains into thoracic duct while right goes straight to venous system. Super helpful when you're trying to figure out lymphatic spread patterns, just work backwards from there.
So the bronchomediastinal trunk is kinda weird - it works totally differently from person to person. Some people have this big robust trunk that drains tons of fluid from their lungs and chest area, while others have these tiny little vessels that barely do anything. The drainage patterns shift around too. Like, one person's trunk might focus more on lung stuff, another person's handles mostly chest structures. Honestly makes you realize how much our anatomy varies! Oh and when you're checking patients, these differences can totally change how diseases show up or get worse.
So the bronchomediastinal trunk is like the main lymphatic drain for your chest area. It pulls lymph from your lungs, the space between them, and some chest wall stuff. Why does this matter? Well, your lungs are constantly getting hit with bacteria and junk from the air you breathe. This system lets your immune cells patrol everything and flag problems. When you get lung infections or - god forbid - something like cancer, doctors can actually predict which lymph nodes will get affected first based on how this drainage works. Pretty clever how it's all mapped out, honestly.
So basically, lung cancers and mediastinal tumors are the big culprits here - they block up the bronchomediastinal trunk and mess with lymphatic drainage. TB can do this too, though you don't see that as much anymore. Surgery's another problem since those vessels are pretty delicate and easy to damage during procedures. What happens is you get fluid backup and your immune system can't clear stuff properly from the chest. If someone keeps getting pleural effusions or weird respiratory infections that won't quit, I'd definitely think about whether their lymphatics got compromised somehow. It's one of those things that's easy to miss but explains a lot once you connect the dots.
For the bronchomediastinal trunk, I'd go with CT contrast first - gives you really solid detail of those lymphatic vessels and how they sit with everything else in the mediastinum. MRI works too, especially T2 sequences since they light up fluid-filled channels nicely. Lymphangiography is technically the gold standard, but honestly it's pretty invasive so most people skip it unless you're dealing with something really complex or prepping for surgery. Ultrasound might catch dilated vessels sometimes, though the location makes it a pain to get good images. CT with contrast is probably your best bet to start.
Honestly, the bronchomediastinal trunk is one of those structures you really don't want to mess with during thoracic cases. It handles all the lymphatic drainage from lungs and mediastinum. Damage it during lung resections and you'll get chylous effusions - not fun for anyone. When you're doing radical lymph node dissections for lung cancer, preserving that lymphatic flow makes a huge difference in recovery times. I actually saw a case last month where we had to ligate it after accidentally nicking it during dissection. My advice? Identify it early and keep your distance. Way easier than dealing with the headache of postop complications.
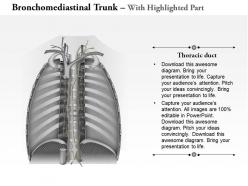
So the bronchomediastinal trunk connects to the main lymphatic vessels - left side usually hits the thoracic duct, right side goes to the right lymphatic duct. It's like local streets feeding into highways, you know? Left side's pretty predictable, joins near the subclavian-internal jugular spot. Right side's more all over the place though. Oh and heads up - if you mess with these during thoracic stuff, you might get chylous leaks. Had a case last month where we didn't map it out first... not fun. So yeah, always check those connections beforehand.
Look out for upper extremity lymphedema and recurrent respiratory infections - that's your big red flag. Surgery, radiation, or cancer can mess up the bronchomediastinal trunk, so lymphatic fluid just sits there instead of draining properly from the lungs. Honestly? This gets overlooked way too often. You'll also see weird stuff like wounds that won't heal after chest surgeries or pleural effusions that are stubborn as hell. Post-surgical patients are especially at risk, along with anyone who's had chest radiation. It's one of those things that should be on your radar more than it probably is.
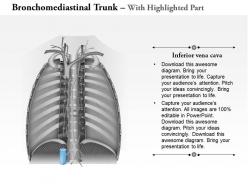
So the bronchomediastinal trunk basically dumps lymph back into your bloodstream through a couple different routes. Right side usually hooks up with the right lymphatic duct first, then hits that venous angle where your jugular and subclavian veins meet. Left side's kinda messy though - sometimes it goes straight to the thoracic duct, sometimes directly to the venous angle. There's honestly a ton of variation between people, which made studying this stuff annoying. But yeah, all that lymph from your lungs and heart area has to get back into circulation somehow.
So if you damage the bronchomediastinal trunk, you're basically asking for lymphatic headaches. The big thing to worry about is chylous effusions - that milky fluid can build up in the pleural or pericardial space, which honestly sucks to deal with after surgery. This trunk handles drainage from lungs, mediastinum, and chest wall, so when it gets messed up during thoracic procedures or central lines, that fluid has nowhere to go. Watch for any weird milky drainage or random effusions post-op. Catching it early saves everyone a ton of hassle later.
So the bronchomediastinal trunk is basically where all the lymphatic drainage from your lungs, heart, and mediastinum meets up - it's like the main highway for fluid. When cancer hits this spot, it's already spread way beyond the original tumor site. Pretty much means the disease has gone from local roads to the interstate, if that makes sense. Doctors will bump you up to a higher stage at that point. Surgery becomes way harder, sometimes impossible to get it all. I think most oncologists would probably pivot to chemo or other systemic treatments instead of trying to cut everything out. It's just too widespread by then.
So the bronchomediastinal trunk can be pretty unpredictable - sometimes it drains straight into the venous angle instead of connecting to the thoracic duct like you'd expect. You might find multiple small trunks instead of one big one too. The left side is honestly where things get messy and don't match what you see in textbooks. During thoracic surgery this stuff actually matters since lymphatic drainage from lungs and mediastinum varies way more than people think. Don't just rely on standard anatomy maps when you're planning procedures because it'll bite you.
So the bronchomediastinal trunk is super variable because of how it develops - multiple lymphatic bits that sometimes fuse, sometimes don't. It's honestly pretty annoying from a surgical standpoint. You'll see it drain into the subclavian vein, jugular, or thoracic duct depending on the patient. Makes planning thoracic cases tricky since textbook anatomy doesn't match reality half the time. That's why I always triple-check the preop imaging for variants before heading into the superior mediastinum. Embryology really did us dirty with this one.
-
Best way of representation of the topic.
-
Informative design.